News & Events
Branch-ostial lesions: easy but tricky
There is no denying that the main target during PCI are significant proximal lesions in the three main coronary vessels (LAD, RCA and LCX), but sometimes we are faced with ostial significant lesions in sizable side branches that shouldn’t be overlooked (especially, OM and diagonals).
We are focusing here on MEDINA 0,0,1 ostial bifurcational affection (the disease is exclusive to the ostium of side branch . The most unfavorable strategy here is just putting the stent flushed at the SB ostium as you will for sure have one of two complications:
- Missing to cover part of the ostium if the stent is less protruded into the Main branch (MB), this uncovered part of the plaque will be a nidus for either thrombosis or re-stenosis.
- The reverse, excessive protrusion of the stent into the MB, this floating stent struts may trigger thrombosis.
The best strategy her is either:
- PTCA then drug-eluting balloon (DEB) to the ostium of SB, especially beneficial if there is a discrepancy of the size and the significance between the MB and SB (ex: A large LAD of more than 4 mm and a relatively narrow diagonal)
Half-culotte technique especially if the sizes and the significance of MB and SB are comparable (LCX and OM for instance): in this technique a longer stent is deployed from the MB to the SB. the length of the part of MB covered by the stent should comply with the length of the available short NC balloon used for post-dilatation and POT (proximal optimization). POT is unequivocally pivotal here to keep the patency of both MB and SB and to remove any struts of the stent facing the blood flow in the MB.
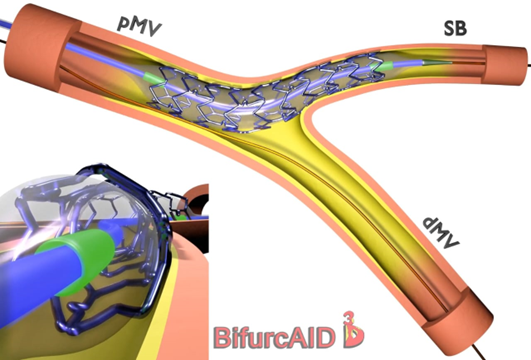
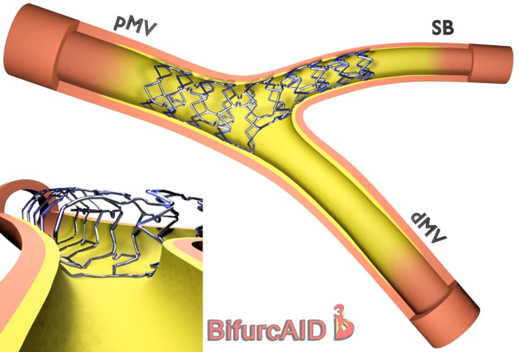
The images are from Bifurcaid 3-D App on google play for android devices, developed by Mount Sinai Universtiy – USA